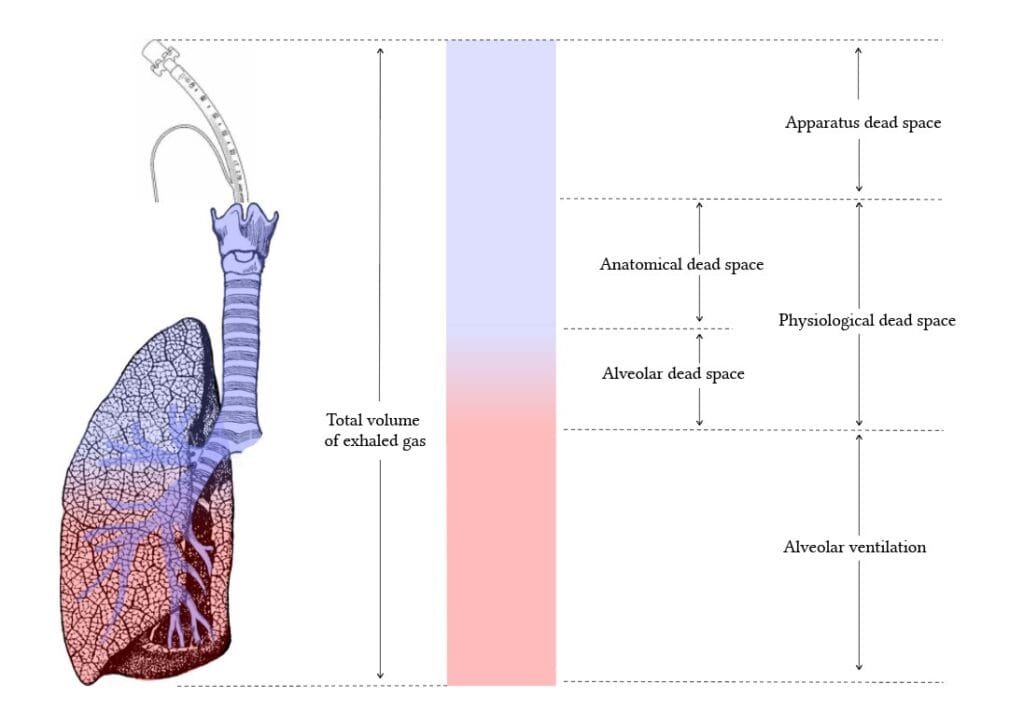
Total dead space (Physiological dead space) = Anatomical dead space + Alveolar dead space.
Anatomical Dead Space
It is constituted by air which is not participating in diffusion. Therefore it is constituted by air present in nose, trachea and bronchial tree (up to terminal bronchioles). Normally it is 30% of tidal volume or 2 ml/kg or 150 ml.
 Anatomical dead space is increased in:
Anatomical dead space is increased in:
i. Old age
ii. Neck extension
iii. Jaw protrusion
iv. Bronchodilators
v. Increasing lung volume
vi. Atropine (causes bronchodilation)
vii. Anesthesia mask, circuits
viii. Intermittent positive pressure ventilation (IPPV) and positive end expiratory pressure (PEEP).
Anatomical dead space is decreased by:
i. Intubation (nasal cavity is bypassed and diameter of tube is less than airway diameter)
ii. Tracheostomy (upper airways and nasal cavity bypassed)
iii. Hyperventilation (decreasing lung volume)
iv. Neck flexion
v. Bronchoconstrictors
Alveolar Dead Space
Constituted by alveoli which are only ventilated but not perfused. It is 60 to 80 ml in standing position and zero in lying position (in lying position perfusion is equal in all parts of lung). It is increased by:
- Lung pathologies affecting diffusion at alveolar capillary membrane like interstitial lung disease, pulmonary embolism, pulmonary edema and ARDS.
- General anesthesia.
- IPPV (Intermittent positive pressure ventilation).
- PEEP (Positive end expiratory pressure).
- Hypotension.
All anesthesia circuits, masks, humidifiers increase the anatomical dead space.
Endotracheal tubes, tracheostomy decreases the anatomical dead space by bypassing the upper airways. All inhalational agents increase both anatomical and alveolar dead space. Anatomical dead space is increased because all these agents are bronchodilators.
Alveolar dead space is increased because of hypotension produced by these agents (V/Q mismatch). Positions during anesthesia especially lateral position causes more ventilation in upper lung (non dependent) and more blood flow in lower lung (dependent lung) so increasing the V/Q mismatch and hence alveolar dead space. Other positions like Trendelenburg, lithotomy also causes the V/Q mismatch.
Anesthesia ventilation techniques like IPPV (Intermittent positive pressure ventilation) and PEEP (Positive end expiratory pressure) increase both anatomical dead space and alveolar dead space.
Anatomical dead space is increased by increasing lung volume and alveolar dead space is increased because of hypotension produced by IPPV and PEEP (compression of venules in alveolar septae and interstitial tissue because of dilated alveoli by PEEP and IPPV leads to decreased venous return and compression of small arteries lead to decrease in pulmonary blood flow.
Both these factors finally decrease the cardiac output and thus causing hypotension).
Secondly, alveolar dead space is also increased by PEEP because normal alveoli are overdistended during PEEP, increasing V/Q mismatch.